27 March 2024 | This Focus Paper analyses the new system for the distribution of the Italian national health service (INHS) financing, introduced in 2023 by the agreement of the State-Regions Conference held on 21 December 2022 and the decree of the Minister of Health dated 30 December 2022. The per-capita criterion, partially weighted to consider the age as a factor influencing the health services consumption, has been joined by other parameters, i.e. mortality under 75 years and some indicators of socio-economic conditions. The Focus Paper sheds some light on the implications of the new allocation mechanism and assesses the distributional impact of the reform.
Article 119 of the Constitution stipulates that the resources granted to local authorities shall be adequate to fully finance the public tasks under their responsibility. This requires defining allocation criteria consistent with expenditure needs.
The standard national health expenditure requirement is defined by Legislative Decree No. 68/2011 – which regulates the determination of standard costs and expenditure requirements in the health sector – as the level of financing of the INHS to which the State regularly contributes. The INHS financing is set by a state law (usually the Budget Law) and by agreements between the state and the regions, although the latter have not always preceded the legal determination of the financing amount and, often, the level of funding has eventually been adjusted. The funds are then distributed among the regions. However, autonomous regions (those with a special statute) finance their own health services autonomously (Sicily only partially) and, therefore, the share allocated to them does not represent a real transfer.
The problem of identifying non-arbitrary criteria – to ensure equal access and efficient expenditure – for the allocation of health care resources affects all decentralised health care systems. In the general run of things, the per-capita criterion is the most frequent one, supplemented by other aspects. The attempt is to allocate funds based upon needs, often using the consumption of health services as a proxy, although this approach brings up some problems: inappropriate consumption, physical or economic barriers to access, lack of awareness of need. Since no estimation method can accurately predict expenditure needs, some degree of uncertainty persists, which can be addressed through different tools, ranging from retrospective renegotiation of funds, the definition of other sources of financing, to rationing of services.
Age is regarded as the main factor determining the health status and health care consumption. The influence of socio-economic conditions is also widely agreed upon. In this respect, premature mortality (below a certain age) is associated with deprivation (used as a proxy for unmet need in the English system).
Even before the recent reform, the system for allocating resources to the INHS was very complex, also because of the coexistence of different distribution mechanisms for different shares of the funding: indistinct funding (not bound to specific objectives), the Innovative Medicines Fund, earmarked resources for the regions or other entities, and the bonus share. The latter, which has increased over the years and amounted to 0.5 per cent of the National Health Expenditure Requirement in 2023, is set aside and then distributed in agreement with the State-Regions Conference, with due consideration of the rebalancing criteria stemming from the negotiations held within the Conference of Regions and Autonomous Provinces. The criteria underlying the distribution of the bonus share are not necessarily disclosed.
For the bulk of the indistinct funding, Legislative Decree No. 68/2011, as amended by Law No. 190/2014, had introduced a transitional regime with a weighting of the per-capita share by age groups, and had indicated as weights to be adopted, as from 2015, those established by Law No. 662/1996. The latter in turn included the resident population, the health care consumption rates by age and gender, mortality rates, additional indicators relating to particular local situations deemed useful for defining the health needs of the regions, and regional epidemiological indicators. Furthermore, Legislative Decree No. 68/2011 provided that the distribution should also consider the path towards improving quality standards through the implementation and application of a system for evaluating and monitoring care and assistance. In practice, the distribution mechanism, which was adopted as a temporary measure, remained in force until 2022.
Weighting by age group ensures additional resources for the areas with a higher proportion of elderly people and reduces the share of resources allocated to Lombardy, Lazio and the large southern regions (except for Sardinia).
As far as the new allocation criteria are concerned, the distributional effects seem to meet the expectations. More specifically, as the mortality parameter is based on premature mortality (albeit with a rather high age threshold of 75) and the additional indicators of peculiar regional situations (relative poverty, low education and unemployment) are interpreted as indicators of socio-economic conditions (deprivation), the new mechanism for allocating resources has generally favoured the southern regions, where deprivation is more widespread, and in particular Campania, which is granted 84 additional million, Sicily (+56 million), Apulia (+45 million) and Calabria (+21 million). Conversely, Lombardy (-71 million), Veneto (-33 million) and Emilia-Romagna (-30 million) were penalised. The deprivation criterion produced the strongest effect.
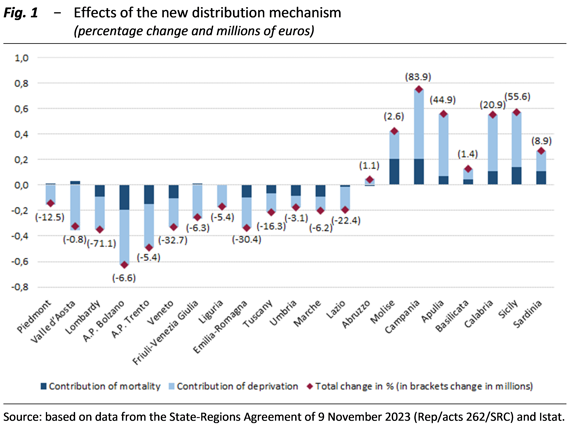
Source: based on data from the State-Regions Agreement of 9 November 2023 (Rep/acts 262/SRC) and Istat.
The result partly neutralises the loss incurred by some regions, particularly Campania and Sicily, as a result of the weighting of the per capita share with consumption by age group, thus rebalancing the allocation of resources in line with the rationale where age is the main factor for determining health status and health expenditure needs, followed by socio-economic conditions. Therefore, including the new indicators in the distribution criteria should ensure a better match between regional health needs and the resources allocated to meet them.
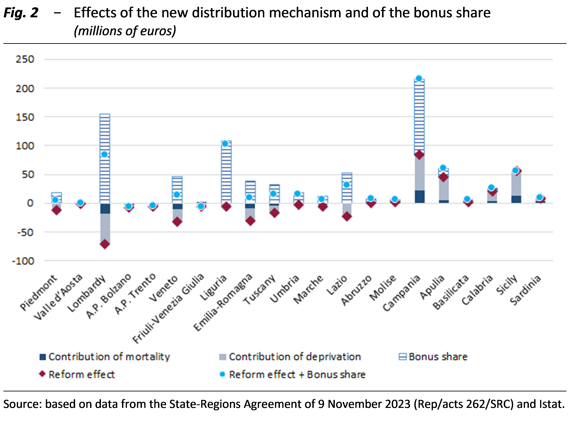
However, it is also worth noting that a significant share of the funding, known as the bonus share, is allocated through negotiations between the regions. These negotiations generally seem to take due account of the negative impacts on some of them stemming from the distribution of the general funding or other causes and to try to mitigate them. This facilitates agreements upon solutions on resource allocation, but it also reduces the transparency of the distribution mechanism. The amount of the bonus share (644 million in 2023) is significant as it represents one third of the funding distributed based on premature mortality and deprivation (1,811 million). It is important to note that this share is allocated on a discretionary basis and can significantly benefit some regions. In 2023, Lombardy, Liguria, and Lazio received 155 million, 108 million, and 53 million respectively. This neutralises the losses incurred due to the new distribution criteria. Campania and Apulia received 131 million and 16 million respectively, consolidating their advantage.
A closer examination of the algorithm used to apply the new criteria highlights some aspects of the new distribution system, not all of which are immediately evident, which become relevant.
First, the overall redistributive capacity of the new criteria, conceived as the total resources shifted by the new system, amounts to 219 million for 2023. This is calculated as the sum of the positive or negative differences between the post-reform and pre-reform results in the various regions. If the share of funding distributed according to the new criteria were to increase by one percentage point, an additional 146 million would be reallocated among the regions. Meanwhile, if only deprivation were considered for distribution purposes, it would be 225 million and considering only mortality would result in 71 million.
Second, the definition of the weights and the system used for aggregating the indicators of relative poverty, low education and unemployment into a sort of deprivation index to be used for distribution purposes implies the double counting of individuals who are deprived according to more than one indicator. Thus, given the aggregation system, the implicit value given by the equal weighting of the three variables reflects the attribution of higher risk to individuals with more than one form of deprivation. However, the aggregation of the three indicators through geometric average allows balancing the lower values of one indicator with the higher values of others.
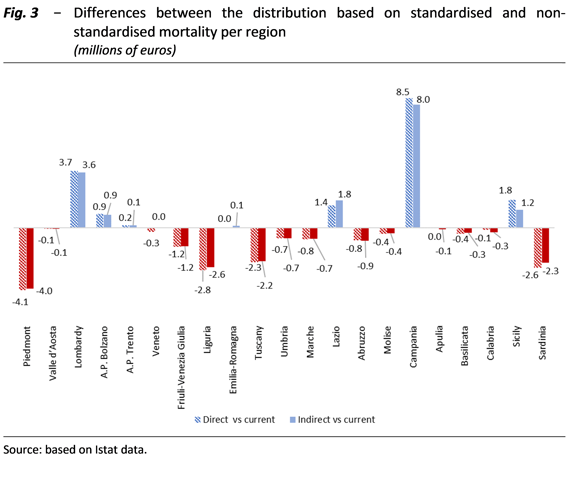
Third, it seems more consistent to take into account the differences in the structure of the population by age group in the various regions, for the distribution purposes based on premature mortality, using standardisation methods that are suitable for neutralising these differences, which, unlike the specific regional mortality rates by age, are not linked to conditions of marginalisation. This would particularly benefit Campania (around 8 million) and Lombardy (3.5 million). On the other hand, the current methodology benefits Piedmont, Liguria, Sardinia and Tuscany.
Lastly, it is worth noting that the other criteria provided for by Law No. 662/1996 and Legislative Decree No. 68/2011 have not yet been included in the distribution mechanism, pending the availability of suitable data and the resolution of privacy-related problems.
Moreover, should the mechanism and parameters adopted for the allocation of resources be reviewed, it could be useful to estimate the joint weights of the age and deprivation variables on the basis of past consumption in order to assess the respective roles of the two determining factors of health expenditure needs, despite the fact that consumption alone does not comprehensively reflect all the needs. In this case as well, the available databases should be supplemented, without prejudice to compliance with the rules on the processing of personal and sensitive data.